A benign cutaneous histiocytoma in a pug
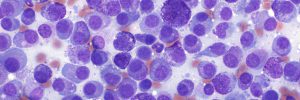
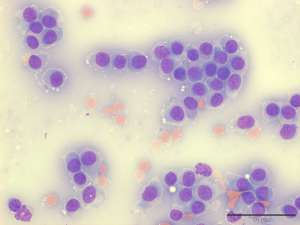
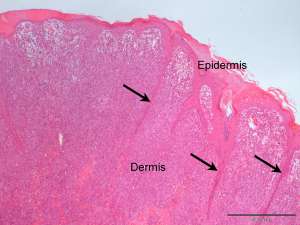
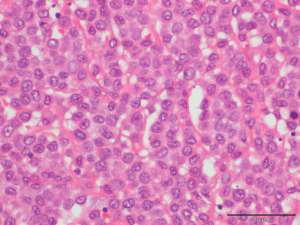
The following are cytological and histopathological specimens taken from a 1cm cutaneous mass on the pinna of a 7-year old pug.
Final Diagnosis
Cutaneous histiocytoma
Discussion
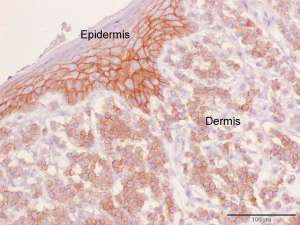
Cutaneous histiocytomas are common benign canine neoplasms. They arise from the epidermal Langerhans cell which is a type of antigen-presenting dendritic cell. They most commonly occur in young dogs however a fair proportion also occur in older dogs and therefore should remain on the differential list for a cutaneous mass, no matter what the age of the dog.
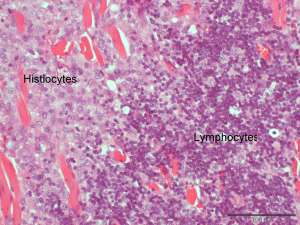
Lymphocyte-mediated regression of these tumours is common and this is why lymphocytes are commonly found in both aspirates and biopsies taken from these tumours. It is also the reason why treatment with immunosuppressive drugs is contraindicated because this may impair or delay the so-called ‘spontaneous regression’. In some cases of regressing histiocytomas, the number of lymphocytes will exceed the number of remaining neoplastic histiocytes, making the diagnosis a bit more difficult. Occasionally, some dogs may develop recurrent and/or multiple histiocytomas and these are usually associated with a lack of immune-response manifested histopathologically by a lack of lymphocytic infiltrate.
Ulceration and/or secondary bacterial infection is a common complication in cutaneous histiocytomas and this often necessitates surgical excision.