Erythema multiforme in a Labrador Retriever
A 1-year-old female Labrador was treated for bilateral otitis externa with a 2 week course of cephalosporins. During the course of antibiotic treatment, multiple regions of cutaneous ulceration developed, particularly affecting the ear pinnae and ventral abdomen. Biopsies from the affected areas (including immediately adjacent non-ulcerated skin) were taken and submitted for histopathology.
Final Diagnosis
Erythema multiforme
Discussion
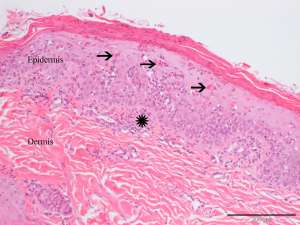
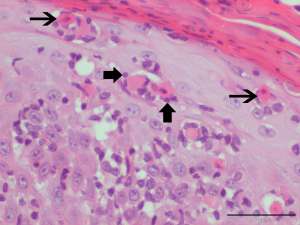
The term erythema multiforme (EM) is used by pathologists to denote the presence of keratinocyte necrosis (apoptosis) in association with lymphocyte satellitosis and essentially denotes an uncommon type of cutaneous reaction pattern. Interface dermatitis (although mild in this case) is also a common finding.
EM can vary from mild and self-limiting to a more severe form of disease which may include signs of systemic illness (e.g. fever). Clinically, cutaneous lesions most commonly affect the ventrum, groin/axilla, oral cavity, mucocutaneous junctions, pinnae and pawpads. Lesions typically begin as papules, circular plaques or targetoid lesions which may ultimately progress to ulceration.
The pathogenesis of erythema multiforme is not fully understood but it is currently believed to represent a T cell-mediated hypersensitivity reaction. Although idiopathic forms exist without a history of known triggers, the majority of cases are linked to a drug hypersensitivity reaction. Infection and neoplasia are considered to be less common triggers of the disease. The most commonly implicated drugs in dogs are antibiotics and include trimethoprim-potentiated sulphonamides, penicillins and cephalosporins. Essentially what happens is that keratinocytes become antigenically altered which results in T cells binding to them and inducing keratinocyte death by apoptosis – this is the interaction which can be appreciated microscopically as ‘lymphocyte satellitosis’. EM occurs rarely in cats and is similarly associated with drug hypersensitivity, although herpesvirus has also been implicated in some cases. Interestingly, herpesvirus infection is a common trigger of mild EM in humans whereas drug hypersensitivity reactions usually account for the more severe form of EM.
Diagnosis is based on the clinical signs, a history of known triggers and histopathology.