Cutaneous epitheliotropic lymphoma in a Cavalier King Charles Spaniel
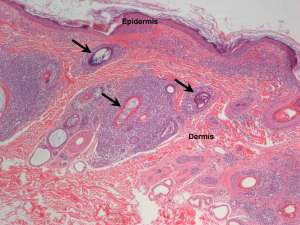
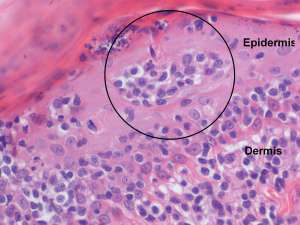
The following are H&E sections of skin biopsies taken from a 6-year-old female CKCS with multiple coalescing cutaneous plaques on the ventral abdomen.
Final Diagnosis
Cutaneous epitheliotropic lymphoma (mycosis fungoides)
Discussion
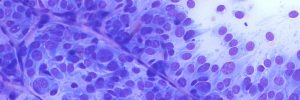
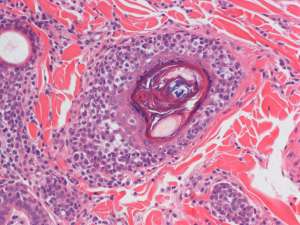
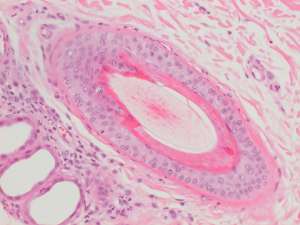
Cutaneous epitheliotropic lymphoma is essentially a T-cell lymphoma in which the neoplastic lymphocytes have a propensity to infiltrate the epidermis and adnexal epithelium. In the majority of cases, the mitotic rate is low (typical of a low grade lymphoma) and this correlates with the slowly progressive nature of the disease. Clinical disease may range from a few months to up to two years, however eventual spread to the regional lymph nodes and internal organs should be anticipated. It is important to remember that epitheliotropic lymphoma is not always restricted to the haired skin and may also involve the mucocutaneous junctions and oral mucosa.
The index of suspicion for epitheliotropic lymphoma is often not high in the clinical setting because the signs are often non-specific and can mimic inflammatory disease.
Broadly speaking, the different clinical manifestations can be divided into four main categories:
- A multifocal to coalescing exfoliative dermatosis with scaling and alopecia
- Solitary or multiple cutaneous plaques or nodules which can mimic other neoplasms
- Concurrent or isolated involvement of the mucocutaneous junctions, particularly the nose, eyelids and lips. At these sites, depigmentation is a main feature that often occurs in conjunction with erythema and erosion. Similar signs can occur with immune-mediated disease that makes clinical differentiation difficult.
- The disease may be restricted to erythema and erosion or ulceration of the oral mucosa, especially the gingiva, palate and tongue. The presence of gingival erythema and/or erosion in the absence of periodontal disease for example should raise the suspicion for epitheliotropic lymphoma.
Confirmation of the diagnosis is by histopathological evaluation and additional evaluation of any enlarged regional lymph nodes (either by fine needle aspirate or histopathology) will help with the initial staging process.